
| What is FMECA in Process Safety? Failure Mode, Effects, and Criticality Analysis (FMECA) is a quantitative risk assessment method used to identify potential equipment failures, analyze their consequences, and rank them based on criticality. Unlike standard FMEA, FMECA assigns a specific “Criticality Number” to each failure mode (Severity × Probability), allowing process safety engineers to prioritize maintenance resources on the highest-risk assets. |
If you work in a plant that handles hazardous chemicals, you already know this truth:
Equipment never just “fails”. It fails in a specific way, for a specific reason, and that failure has a specific impact.
Failure Mode, Effects and Criticality Analysis (FMECA) is a structured way to map all of that out before something goes wrong.
This systematic methodology is used to identify potential equipment or system failures, evaluate their effects, and quantify their criticality to prioritise risk mitigation. In process safety management, FMECA strengthens risk assessments by providing a structured, bottom-up approach that complements hazard analysis techniques such as HAZOP and SIL/LOPA.
FMECA supports Process Safety Management (PSM) by exposing weaknesses in equipment reliability, highlighting safety-critical components, and improving hazard identification and mechanical integrity programmes. It is widely used across the lifecycle of a process, from early design to operation and decommissioning.
What Is FMECA?
|
FMECA = FMEA + How worried should we be? FMEA (Failure Mode & Effects Analysis) asks: – How can this thing fail, and what happens if it does? FMECA asks one more question: – And how critical is that failure, considering how bad it is and how likely it is? |
So, with FMECA, you don’t just list failures. You rank them so you know where to focus your time, money, and attention.
In process safety, that’s powerful because a small piece of equipment (a valve, a seal, a transmitter) can be the difference between normal operation and a major accident.
The History
FMECA evolved from early aerospace and defence reliability methods, formalised in MIL-STD-1629A, which introduced a structured process for identifying failure modes and ranking their criticality. Over time, the method has been adopted in chemical processing, energy systems, and industrial safety applications due to its rigorous, traceable approach.
Unlike FMEA, which stops at failure effects, FMECA adds criticality analysis, enabling a prioritised ranking of risks using severity and probability. This makes it valuable for managing both process safety and operational risks, where the consequences of failure can involve toxic release and fire/explosion, as well as significant asset damage, unplanned downtime, or production losses.
What is the difference between FMEA and FMECA in process safety?
| Aspect | FMEA | FMECA |
| Goal | List failure modes and effects | List failure modes and effects, and rank them by criticality. |
| Nature | Mostly qualitative (descriptive) | Semi-quantitative / quantitative |
| Output | Risk Ranking Table | Risk Priority Number (RPN), Criticality index/zone, top critical items |
| Use case | General quality, reliability | Safety-critical systems, high-consequence plants |
Why FMECA Is Important in Process Safety
In process plants, we care about more than downtime. We care about:
- Loss of containment (toxic release, flammable release)
- Fire and explosion risk
- Environmental impact (spills, long-term contamination)
- Long outages and costly repairs
FMECA helps you:
1.Spot weak links in safety-critical equipment
- Pumps that tend to leak
- Valves that can fail stuck open
- Instruments that drift and defeat a safety function
2. Prioritise what really matters
Instead of treating every failure equally, you focus on items that are:
- High severity (big consequences if they fail)
- High likelihood (they actually do fail in the real world)
3. Strengthen your PSM elements
FMECA feeds into:
- Hazard identification and risk assessment (HAZOP, SIL/LOPA)
- RAM Analysis
- Mechanical integrity / reliability programmes
- Safety-critical element (SCE) management
- Inspection and maintenance strategies
Process safety demands a strong understanding of how systems can fail and how those failures propagate. FMECA provides a structured, equipment-level analysis that helps identify vulnerabilities in safety-critical equipment, instrumentation, and process barriers.
By quantifying criticality, FMECA allows organisations to focus resources where they matter most: equipment with both high severity consequences and high likelihood of failure. This aligns with recognised engineering principles of risk reduction and mechanical integrity.
A simple example: FMECA on a toxic transfer pump
Imagine you’re analysing a pump that transfers a toxic solvent from storage to a reactor.
Function:
Transfer solvent at x m³/h from Tank A to Reactor B at y bar.
Some possible failure modes:
- Seal failure → external leak
- Pump stops → underfeed to reactor
- Pump runs with no flow → overheating, damage
- Valve downstream stuck closed → overpressure on discharge
For each failure mode, FMECA asks:
- How does it fail? (Failure mode: e.g., seal leak)
- What happens? (Effects: leak to atmosphere → toxic exposure or repair time leading to significant downtime and production loss)
- Why does it fail? (Causes: seal wear, poor lubrication, misalignment)
- How bad is it? (Severity: from minor to catastrophic)
- How often might it happen? (Probability: based on data / judgement)
- How critical is it? (Criticality: combination of severity + probability)
If “seal failure → toxic leak” scores high severity and credible probability, it lands in a high criticality zone and becomes a priority for:
- Better seal selection or double seals
- Leak detection
- More frequent inspection
- Clear response procedures
The FMECA Methodology
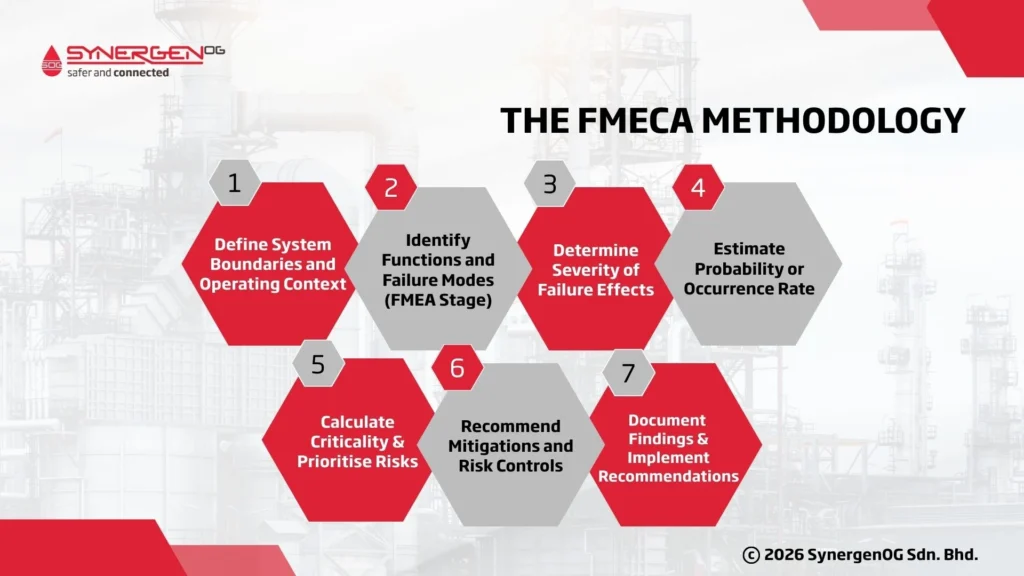
1. Define System Boundaries and Operating Context
FMECA begins with a clear definition of the system under review, including process conditions, design intent, interfaces, assumptions, and environmental factors. This ensures the analysis is accurate and avoids missing critical elements.
Be clear about what you are analyzing:
- Which system? (e.g., Caustic transfer system from tank to neutralization unit)
- Where does it start and end? (pumps, piping, valves, instruments, control system)
- Operating conditions (temperature, pressure, flow, phases)
- Interfaces (upstream/downstream systems, utilities, safety systems)
2. Identify Functions and Failure Modes (FMEA Stage)
The FMEA stage identifies component functions, failure modes (e.g., leak, rupture, blockage, drift), causes, and immediate effects. This is typically performed using worksheets or software, supported by engineering judgement and data sources.
Typical failure modes in process equipment:
- Leak/rupture
- Blockage
- Stuck open/stuck closed
- Fails to open/fails to close
- Drifts out of range (for instruments)
- Spurious trip / no trip
3. Determine Severity of Failure Effects
Severity reflects the consequences of each failure mode, including safety impacts, environmental effects, operational disruption, or equipment damage. Severity scales are defined to maintain consistency across the FMECA.
A simple four-level severity scale for process safety,
- Severe – Potential for multiple fatalities, major offsite impact, or major long-term environmental damage, or catastrophic production loss (e.g., total plant shutdown for >1 month).
- Major – Single fatality or serious injury, significant release, significant plant damage
- Moderate – Recordable injuries, moderate release, limited equipment damage, production loss
- Minor – No injury, small spill, minor downtime
The exact definitions should match your company’s risk matrix, so FMECA results tie directly into your existing risk framework.
4. Estimate Probability or Occurrence Rate
Probability is estimated using failure rate data, equipment histories, vendor documentation, or reliability databases such as MIL-HDBK-217F. Accurate probability estimation ensures meaningful criticality ranking.
Sources you can use,
- Historical failure data from your CMMS / maintenance system
- Vendor reliability data and OEM manuals
- Industry reliability handbooks/databases
- Engineering judgement (with clear assumptions)
5. Calculate Criticality and Prioritise Risks
Criticality analysis combines severity with occurrence (and sometimes detection) to determine the relative importance of each failure mode. This results in ranking charts, matrices, or numerical criticality indices used for decision-making.
Criticality = f (severity, probability)
You can do this in three ways:
1.Simple risk matrix (qualitative)
- Plot severity on one axis, probability on the other
- Classify each failure mode into zones: Low / Medium / High / Extreme
2. Semi-quantitative scoring
- Assign numerical scores (e.g., 1–5) for severity and probability
- Multiply or use a matrix to assign a criticality score
3.Full quantitative analysis (when data allows)
- Use failure rate, failure mode ratios, and mission time as in classic FMECA standards for highly critical systems (e.g., offshore, aerospace).
The output you want is a ranked list of failure modes from most critical to least.
6. Recommend Mitigations and Risk Controls
Mitigation measures may include engineering design improvements, redundancy, enhanced instrumentation, inspection intervals, maintenance tasks, alarms, or procedural controls.
7. Document Findings and Implement Recommendations
Documented FMECA results are incorporated into risk registers, maintenance plans, asset integrity strategies, and management of change (MOC) systems to ensure ongoing control of critical risks.
Best Practices of FMECA
A high-quality FMECA requires disciplined facilitation, a multidisciplinary team, validated data, and clear rating criteria. Teams should include process engineers, reliability specialists, operators, maintenance personnel, and safety professionals.
Consistency in scoring severity, probability, and criticality across different systems is essential to maintain objectivity and prevent bias. Aligning scales with corporate risk matrices helps integrate FMECA outputs into wider risk-management processes.
FMECA should not be viewed as a one-off activity; instead, it must be updated when design changes, incident learnings, or new data arise. This ensures the analysis remains accurate throughout the asset lifecycle.
Conclusion
FMECA is not just a reliability calculation tool from aerospace standards. It’s a very practical way to find and fix the weak links in your process safety barriers. Its structured approach aligns strongly with recognized PSM frameworks and provides a quantitative foundation for risk prioritization.
If you:
- Define your system clearly
- Involve the right people
- Keep the scoring simple and aligned with your risk matrix
- And, most importantly, follow through on the actions
…then FMECA becomes a powerful ally in preventing catastrophic events and running a safer, more reliable plant.
To learn more about FMECA training and how SynergenOG can help you with FMECA studies enquire now.