In July 2023, a catastrophic series of explosions and fires struck Dow Chemical Company’s Glycol II plant in Plaquemine, Louisiana, releasing more than 31,000 pounds of toxic and highly flammable ethylene oxide (EtO). The incident triggered a shelter-in-place order for nearby residents and caused severe damage to the facility.
The U.S. Chemical Safety and Hazard Investigation Board (CSB) recently released its final investigation report, shedding light on a cascading series of operational and design failures.
At SynergenOG, we reviewed the CSB’s findings from the standpoint of brownfield process safety. For operating facilities, this incident is a reminder that startup readiness, inerting integrity, and relief-system design must be systematically verified rather than assumed. That is where disciplined brownfield safety studies and reviews become critical.
What Happened at the Dow Plaquemine Facility?
According to the CSB, the incident sequence began when portable work lights used during the May 2023 turnaround were inadvertently left inside the reflux drum. Over time, those lights degraded in ethylene oxide service, and debris from the lights travelled downstream.
What the CSB Determined as Cause and Contributing Factors
The CSB determined that the cause of the incident was the puncture of a rupture disc by metal debris, which allowed ethylene oxide to enter piping that contained air, ignite, and propagate into the reflux drum.
The Safety Issues Identified by CSB
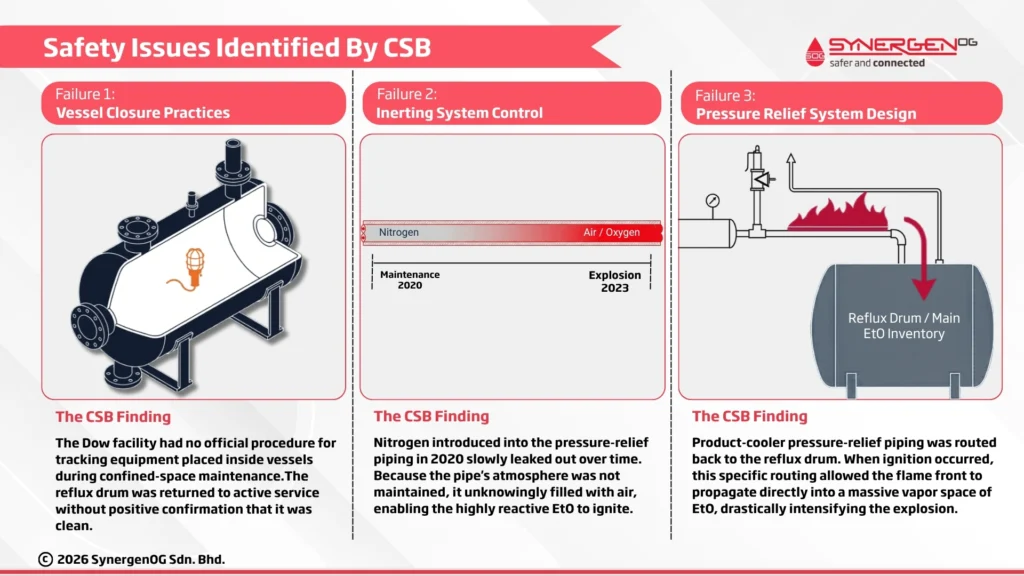
The CSB investigation identifies three principal safety issues: “Vessel Closure Practices,” “Inerting System Control,” and “Pressure Relief System Design.” These findings provide a more accurate framework than describing the event as five separate root causes.
-
Vessel Closure Practices
The CSB states that the incident began when portable work lights were “inadvertently left behind in a reflux drum” during turnaround work. The report further states that Dow’s vessel closure process had “no official procedure in place” for tracking equipment placed inside a vessel during maintenance and inspection activities requiring confined-space entry. The CSB also found that Dow’s vessel closure process and practices “did not adequately identify whether the reflux drum was clean” before startup.
This is a classic startup-readiness failure. A vessel was returned to service without positive confirmation that it was clean and free of foreign materials, and the overlooked items ultimately initiated the event sequence.
SynergenOG’s Role in such scenarios: We help facilities strengthen this type of safety gaps through MOC Reviews and rigorous Pre-Startup Safety Reviews (PSSR). By ensuring that every checklist is scientifically sound and strictly followed, we prevent operational blind spots. Furthermore, our Process Safety Awareness Training helps instill a proactive safety culture where procedures are respected and verified at every level.
-
Inerting System Control
The Failure: The CSB found that nitrogen had been introduced into the pressure-relief piping during maintenance activities in 2020, but the nitrogen “slowly leaked out over time” and the piping “unknowingly filled with air.” The report states that Dow “did not adequately monitor or maintain the inert atmosphere” of that piping segment to ensure that inerting persisted. The CSB news release likewise states that deficiencies in inerting-system control enabled the ethylene oxide to ignite.
For a highly reactive material such as ethylene oxide, this is a critical control failure. Inerting cannot be treated as a one-time condition; it must be maintained and verified during operation where the hazard demands it.
SynergenOG’s Role in such scenarios: Our core expertise lies in facilitating rigorous Process Hazard Analysis (PHA), including HAZID and HAZOP studies. During these sessions, our experienced facilitators actively challenge the design of inerting systems, ensuring that passive assumptions (like “the pipe will stay inert”) are replaced with active, alarmed, and monitored engineering controls.
-
Pressure Relief System Design
The CSB found that the product-cooler pressure-relief piping was vented back to the reflux drum, which allowed the flame front to propagate into the drum’s vapor space and intensified the event. The report states that Dow could have modified the system when the product cooler was replaced in 2010 to eliminate the thermal-expansion hazard and remove the need to vent ethylene oxide into the reflux drum. The CSB concluded that this design “contributed to the severity” of the incident.
This is not just a relief-path issue; it is an inherent-safety and consequence-escalation issue. A relief configuration intended to manage one scenario ended up creating a pathway for flame propagation into a much larger ethylene oxide inventory.
SynergenOG’s Role in such scenarios: While relief system sizing is typically the domain of design and project engineers, SynergenOG plays a vital role in challenging these designs during HAZOP studies. We bring an independent, critical eye to ensure that relief paths do not introduce secondary hazards and strictly adhere to API and NFPA standards.
Why this Incident Matters for Brownfield Process Safety
For brownfield facilities, the Plaquemine incident demonstrates how a maintenance error, degraded inerting integrity, and a legacy relief design can align into a catastrophic process event. The CSB findings reinforce that process safety in operating plants depends on disciplined vessel closure, verified startup readiness, active inerting control, and periodic re-examination of older design decisions during modifications and revalidations.
How SynergenOG Helps Prevent Similar Incidents
SynergenOG supports clients with practical process safety services for operating facilities and brownfield projects, including:
- HAZOP and HAZID facilitation
- Process Hazard Analysis (PHA)
- Management of Change (MOC) reviews
- Pre-Startup Safety Reviews (PSSR)
- Process safety awareness training
- Brownfield risk identification and mitigation
Our role is to help clients identify hidden escalation pathways, challenge assumptions embedded in operating practice and legacy design, and implement safeguards that remain effective in the field.
Conclusion
The CSB’s final report on the Dow Plaquemine explosion identifies three core safety issues: vessel closure practices, inerting system control, and pressure-relief system design. Together, those failures allowed a seemingly localized problem to escalate into a major explosion and toxic ethylene oxide release. For brownfield facilities, the lesson is clear: process safety depends on disciplined verification, not assumption.
References:
- https://www.csb.gov/assets/1/6/dow_investigation_report-final_%28002%29.pd
- https://www.csb.gov/us-chemical-safety-board-releases-investigation-report-on-the-2023-explosion-and-toxic-ethylene-oxide-release-at-dow-plant-in-plaquemine-louisiana/